Get My One-Page Checklist
12 Signs Shame May be Present in Your Counselling Sessions
Shame is one of the most painful and complex emotional experiences your clients may bring into the counselling room. It frequently sits beneath presentations of anxiety, depression, addiction, perfectionism, eating difficulties, anger, relationship struggles and trauma responses. Unlike many other emotions, shame often remains concealed. Clients may not name it directly; instead, you may observe withdrawal, harsh self-criticism, defensiveness, minimisation or a persistent belief that they are “not good enough”.
At its core, shame is not about behaviour but about identity. Where guilt says, “I did something wrong,” shame says, “There is something wrong with me.” This distinction is clinically significant. Guilt can motivate repair and relational reconnection. Shame, by contrast, tends to lead to hiding, self-attack or emotional withdrawal.
Working effectively with shame requires thoughtful pacing, emotional attunement and a therapeutic relationship grounded in safety and non-judgement. When shame is met with empathy and steadiness, it begins to soften. When it is overlooked or inadvertently reinforced, it becomes more deeply embedded.

This article explores how shame manifests in practice, how it develops, and how you can work with it sensitively and effectively in your clinical work.
12 Signs Shame May be Present in Your Counselling Sessions
By engaging with this material, you will be able to:

Shame rarely presents itself explicitly. More often, it emerges through subtle relational shifts and defensive patterns. You may notice clients apologising excessively, minimising their distress, avoiding eye contact, speaking quietly or withdrawing socially. Some struggle with intimacy and vulnerability, while others become defensive, dismissive or irritable when they perceive challenge or criticism. Achievements may be dismissed as insignificant, and perfectionistic or people-pleasing tendencies may dominate.
At times, shame hides behind competence. A client may appear confident, articulate and successful while privately experiencing a deep sense of defectiveness. Others may feel chronically stuck in self-blame that resists rational reframing. In both cases, shame operates at the level of identity rather than behaviour.
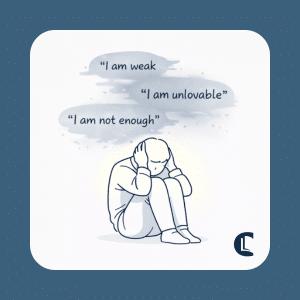
Shame tends to follow a self-reinforcing sequence. A trigger such as criticism, rejection, conflict, failure or a painful memory activates identity-based thoughts – “I am weak”, “I am unlovable”, “I am not enough”. A protective response then emerges, perhaps withdrawal, anger, over-control or emotional numbing. This brings temporary relief, yet the underlying shame remains unexamined and therefore strengthened.
Where clients have experienced repeated invalidation, humiliation or rejection, this pattern can become deeply embedded. Helping clients recognise the cycle allows them to step outside it with greater awareness and choice.
Many clients struggle to identify shame directly. Introducing it tentatively and collaboratively can reduce its intensity and foster safety. Gentle language is essential:
When shame is named within a safe therapeutic relationship, it often begins to lose its secrecy and power. The aim is not to impose an interpretation, but to offer language that may help the client make sense of their experience.
Shame is frequently felt in the body before it can be articulated in words. Clients may describe tightness in the chest, nausea or heaviness in the stomach, heat rising in the face, or a powerful urge to shrink, curl up or disappear. Attending to these sensations can support emotional integration and reduce dissociation.
You might ask, “Where do you notice that feeling in your body?” or “What happens inside as you say those words?” Inviting clients to describe the physical qualities of the experience – its weight, shape or movement – can help anchor them in the present moment. Such work aligns with trauma-informed and embodied therapeutic approaches.
Deeply embedded beliefs sustain shame, often formed in early relational contexts. These beliefs may feel unquestionably true to the client:
Bringing these beliefs into awareness is a vital step. Once named, they can be explored, contextualised and gently challenged. Without conscious recognition, they continue to shape behaviour and relationships outside awareness.
Shame is rarely inherent; it is learned within a relationship. It commonly develops in environments characterised by criticism, humiliation, emotional invalidation, coercion, conditional approval or experiences of being treated as “different” due to identity, culture, neurodivergence or disability.
Exploratory questions may include:
Viewing shame through a developmental lens enables clients to reframe it as an adaptive response to earlier relational experiences rather than as evidence of personal defectiveness. Attachment theory (Bowlby, 1969) and relational approaches such as Erskine’s work on relational needs (Erskine, Moursund & Trautmann, 1999) provide a useful theoretical foundation for this understanding.
A central task in shame work is helping clients disentangle who they are from what has happened to them. Clients often equate painful experiences – or survival strategies developed in response to them – with their core identity.
Interventions might include:
Such reframing supports the development of self-compassion and reduces internalised self-criticism. Compassion-focused approaches (Gilbert, 2009) can be particularly valuable in strengthening this aspect of the work.

Shame rarely exists without protection. Perfectionism, overachievement, people-pleasing, withdrawal, anger, emotional numbing, and rigid control often function as strategies designed to prevent further exposure or rejection. While these patterns may now limit growth or connection, they often originated as attempts to survive difficult relational environments.
Reframing these strategies as adaptive rather than pathological can reduce self-judgement. For example: “his strategy may have helped you survive something very challenging.” When protection is acknowledged respectfully, clients are more willing to examine whether it remains necessary.
Shame can be profoundly overwhelming. Clients may dissociate, shut down, experience panic or become acutely distressed when shame is activated. Effective shame work requires careful pacing and attention to emotional regulation. This may involve slowing the exploration, seeking explicit consent to continue, using grounding techniques and monitoring signs of overwhelm.
Shame work is seldom about pushing through intensity. Rather, it is about establishing sufficient relational safety for clients to remain present with their experience without becoming flooded.
Shame diminishes in the presence of acceptance. Clients often begin to heal when they feel seen and understood without fear of rejection. Your warmth, steadiness and non-judgemental stance are not adjuncts to the work; they are central to it.
Key therapeutic qualities include empathy, emotional calmness, genuine curiosity, respect for pacing and validation without rescuing. Normalising shame as part of the human condition can also reduce isolation.
It is important to recognise that shame can evoke powerful countertransference responses. You may notice discomfort, rescue impulses, frustration or even self-doubt. Ongoing supervision and reflective practice are therefore essential.
Reflective questions for your development might include:
12 Signs Shame May be Present in Your Counselling Sessions
Guilt focuses on behaviour and the sense that “I did something wrong,” which can encourage repair and reconnection. Shame, however, relates to identity and leads clients to believe “there is something wrong with me,” often resulting in withdrawal, hiding, or self-criticism.
Shame rarely appears directly and is often seen through behaviours such as avoiding eye contact, apologising excessively, minimising distress, withdrawing socially, or showing strong perfectionistic or people-pleasing patterns. These responses often reflect a deeper sense of personal defectiveness or not feeling “good enough.”
Working with shame requires a safe, non-judgemental therapeutic relationship where the feeling can be introduced gently and explored at a careful pace. Empathy, emotional attunement, and helping clients separate their identity from painful experiences can reduce shame’s intensity and support greater self-compassion.
Shame thrives in secrecy and silence. It attaches to identity and shapes how clients view themselves and relate to others. When left unaddressed, it perpetuates cycles of withdrawal, perfectionism, anger and emotional numbing.
Your role is not to eradicate shame forcefully, but to create the relational conditions in which it can be named, understood and held safely. Through careful pacing, compassionate curiosity and emotional steadiness, you support clients in separating their inherent worth from their painful experiences.
Healing often begins when shame is met with acceptance rather than judgment.
Bowlby, J. (1969). Attachment and Loss: Vol. 1. Attachment. London: Hogarth Press.
Erskine, R. G., Moursund, J. P., & Trautmann, R. L. (1999). Beyond Empathy: A Therapy of Contact-in-Relationship. Philadelphia: Brunner/Mazel.
Gilbert, P. (2009). The Compassionate Mind. London: Constable.
Transparency note
This article was written and reviewed by human contributors. AI was used as a supportive tool to assist with formatting, layout clarity, and language refinement. All content, interpretations, and ethical positions were created and checked by the authors.
Counselling Tutor provides trusted resources for counselling students and qualified practitioners. Our expert-led articles, study guides, and CPD resources are designed to support your growth, confidence, and professional development.
👉 Meet the team behind Counselling Tutor
Notice any broken link or issues with this resource? Kindly let us know by email
Email us